Blog
Parkinson’s hits minorities in Great Britain

Jun
In the last study Published in the journal Scientists used data from the East London Parkinson disease project to compare the clinical results of Parkinson’s disease (PD) Various ethnic origin in Great Britain. Research results have shown that patients from Southern Asia and Black PD achieved much worse assessment of motor results than their white counterparts.
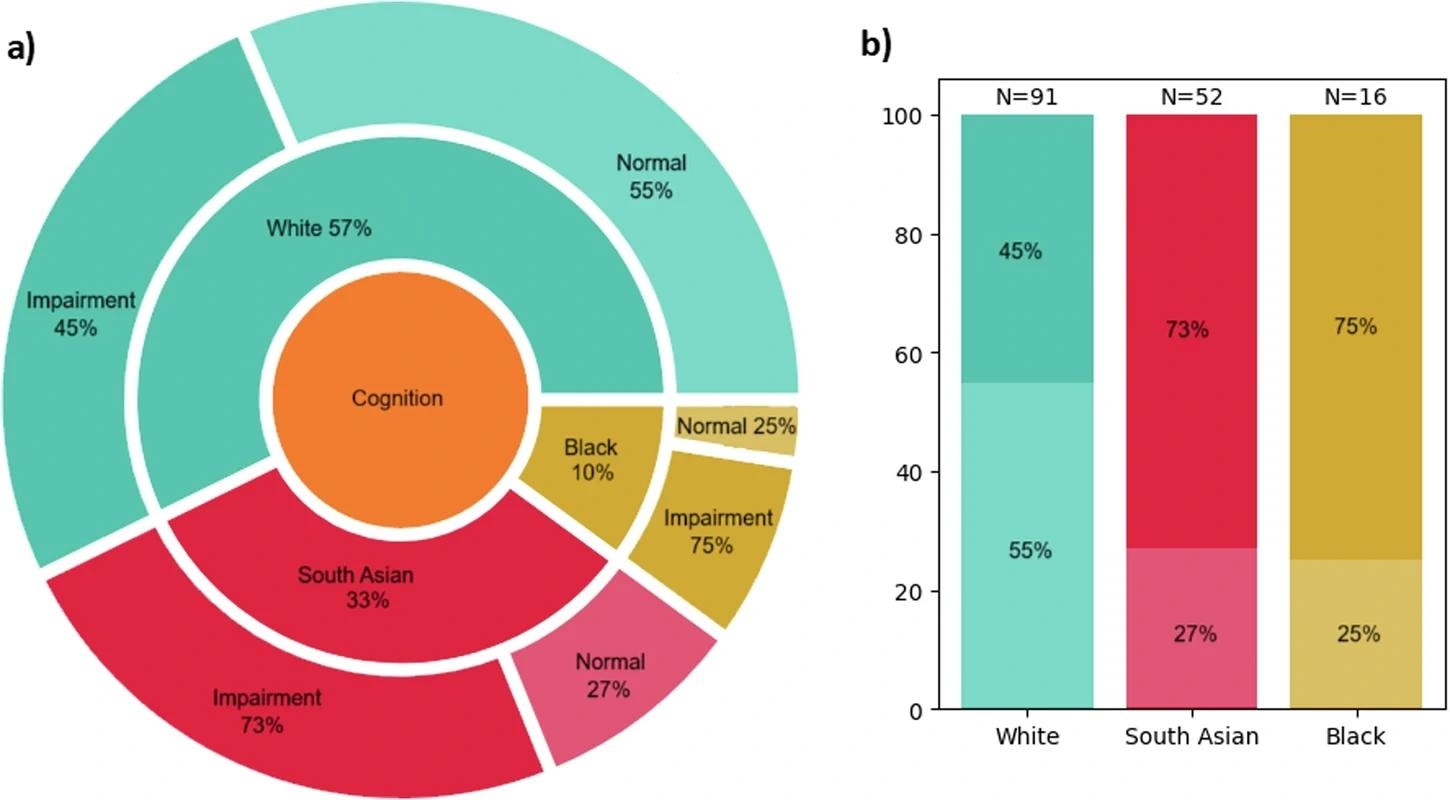
Cognitive impairment was similarly much more widespread in minority patients (75% black, 73% of South Asia) compared to white (45%). Although there was poor evidence that patients from South Asia had a slightly earlier age of symptoms, time from the occurrence of symptoms to diagnosis It turned out to be similar in all groups. These discoveries emphasize the urgent need for policy reform in the field of more integration neuronouka studies and suggest that factors beyond diagnostic access can cause these discrepancies in insufficiently represented populations.
Background
Parkinson’s disease (PD) is a neurodegenerative disorder best known for the progressive exacerbation of motor symptoms, including tremor, stiffness and slow movement. However, PD also involves a wide range of infinity complications, such as cognitive impairment.
The decades of clinical and genetic trials have significantly contributed to the scientific understanding of PD results and genetic predispositions. Recent technological progress, including new generation multiom tools and statistical models supported by artificial intelligence (AI), developed our understanding of PD pathophysiology through jumps and borders.
Unfortunately, most of what we know about the disease comes from research on mostly white Western European populations. These populations are genetically separate and usually more wealthy and educated than South Asian minorities, black and other ethnic minorities.
Lack of ethnically diverse Kohort left key questions unanswered: does the PD manifest itself differently in insufficiently represented groups? Are patients from racial minorities more seriously affected or simply diagnosed, and therefore treated later? Because modern medicine allows the global population to be old, understanding how Parkinson develops in various racial and cultural contexts is necessary for the accuracy of research and building the healthcare system that serves all patients.
About the study
This study uses data from the Eastern London Parkinson disease project, one of the most ethnically diverse groups of urban population, to explain the differences in the age in diagnosis and clinical results of the PD between white, South Asian groups and black ethnic groups. The study uses the design of case control and collected data in many community health services clinics and the National Health Services (NHS) in 2019-2024.
Participants covered by the study were classified as “cases” (MDS 2015 confirmed by PD diagnosis) or “control” (volunteers adapted at the age of neurological disease). The collected data included demographic information (age, gender, ethnic origin and education status), medical history (including diagnosis and PD treatment) and economic variables.
Clinical assessments were carried out using previously approved and standardized diagnostic tools, such as Unified Parkinson’s Scale (UPDRS), to assess the motor function. Cognitive performance was assessed by means of memory tests, attention and executive functions, mainly using Montreal cognitive assessment (MACA).
Comparisons between groups were made using t, χ tests2 Tests, Manna-Whitney tests and Fisher’s thorough tests. Logistic regression models were used to identify the clinical power of PD results. All models have been adapted to misleading demographic, medical and socio -economic variables, especially age, sex and the duration of the disease.
Research results
After excluding patients with “secondary parkinsonism”, an alternative neurological diagnosis or movement, as well as people providing incomplete initial data, the final research group included 218 PD patients, and 90 healthy controls (total n = 318; 37% of women), most of which (64% control, 50% of patients) belonged to ethnic groups. Bangladesh (49%) and Czarni Africans (71%) were dominant ethnicities in South Asian and black podcohorts, respectively.
Age in the analysis of the occurrence of symptoms revealed poor evidence that patients from South Asia developed PD a little earlier (59.2 years) than their white (62.6 years) or black (64.4 years). Most importantly, the time from the occurrence of symptoms to diagnosis was similar in all three ethnic groups that noticed that the authors were a positive discovery suggesting equivalent access to basic healthcare and awareness of PD symptoms in Eastern London.
Patients from South Asian and black origin had much worse disorders of the society movement – Unified Parkinson’s Diseads Rating Skaals (MDS -PdRS) than their white counterparts (42.2, 47.0 and 35.2, respectively). Objective motor assessments, such as a brain test, also showed worse performance in patients from South Asia, although the authors have noticed that factors such as low ability to use a computer can affect these specific results.
The cognitive impairment showed an also striking division between white and minority groups: 75% of black patients and 73% of patients from South Asia showed cognitive dysfunction, compared to only 45% of white patients. This included problems with memory, planning and visual and spatial reasoning, significantly impairing the quality of life (QOL). In addition, the burden of certain infinity symptoms differed, with patients from South Asia reported worse depression and sleep quality, and black patients show a more significant fragrance identification deficit compared to white patients. However, the authors of the study added an important reservation: it has been shown that the cognitive test used to have languages, reading and cultural prejudices, and emphasized that such screening tools developed in white, English -language countries may not be most suitable for different populations without cultural adaptation.
Conclusions
This study provides clear evidence that PD affects racial groups differently, and the authors suggest that more severe motor and cognitive results may occur in patients with black and South Asian compared to white. In this way, this question the long -term assumption that Parkinson is uniform in racial groups, limiting the global generalization of white -oriented PD knowledge.
It seems that these differences exist despite a fair time to diagnosis, and the article suggests that they can be directed by various factors, such as unchanged genetic or environmental influences or higher dissemination of concomitant diseases, such as type 2 diabetes in patients from South Asia. Although further research is needed to determine the causes of the basics, the results emphasize the need for ethnically adapted screening protocols and care that take into account these differences.
Reference to the journal:
- Zirra, A., Dey, KC, Camboe, E. et al. Parkinson’s disease design in East London-Conducting Parkinson’s disease control in a variety of population. Parkinson NPJ disease. 11, 172 (2025), DOI: 10.1038/S41531-025-01031-X, link to publication: https://www.nature.com/articles/s41531-025-01031-X